Histophysiological signs of cellulite
Other signs of cellulite are not visible topographically but may be occurring sub-dermally. Several different mechanisms involving metabolism and physiology are known to contribute to the histopathology of cellulite. These signs appear successively.
- Fat deposition: Not strictly related to cellulite however an aggravating factor is excess fat. Fat in the women, especially deposits in specific sites in a specific manner within adipocytes that appear as bubbles.
- Changes in the connective tissue matrix:It includes collagen and elastin fibers that provide the matrix with flexibility and strength. Within cellulite tissues, is seen a proliferation of these fibers, changing the tissue architecture.
- Alteration of Lymphatic system: The study of ultrastructure biopsies reveals that certain remodeling of the lymphatic system occurs in the localized affected area. This system of vessels that serve to collect excess fluid seeped through the blood vessels back into circulation, is altered by the edema pressure. Obstruction in this system also appears to be responsible for developing cellulite.
- Remodeling of Microcirculation: The edema at the site of cellulite results in congested microvasculature. This constriction in the blood vessels results in a reduced inflow at the site. This manifests as the decreased temperature in the local region as seen by infrared imaging.
- Changes in interstitial fluid: The leaked fluid from the small capillaries accumulates in the spaces surrounding the cells. In microscopic studies, the cellulite tissue is found to have an increased percentage of protein in this fluid. Also, increased pressure of this fluid is recorded.
- Edema: Cellulite is also referred to as Adiposis edematosa. There’s has been found a greater concentration of glycosaminoglycan. Belonging to the family of biomolecules called mucopolysaccharides, they tend to attract water. This localized water retention leads to a swollen appearance upon gross inspection and edema seen microscopically.
- Inflammation: Some research claims to have detected inflammatory cells and other inflammatory changes at the site. This leads to the theory of affiliating cellulite to a mild chronic inflammatory process. However, it has not yet been declared a definite presentation.
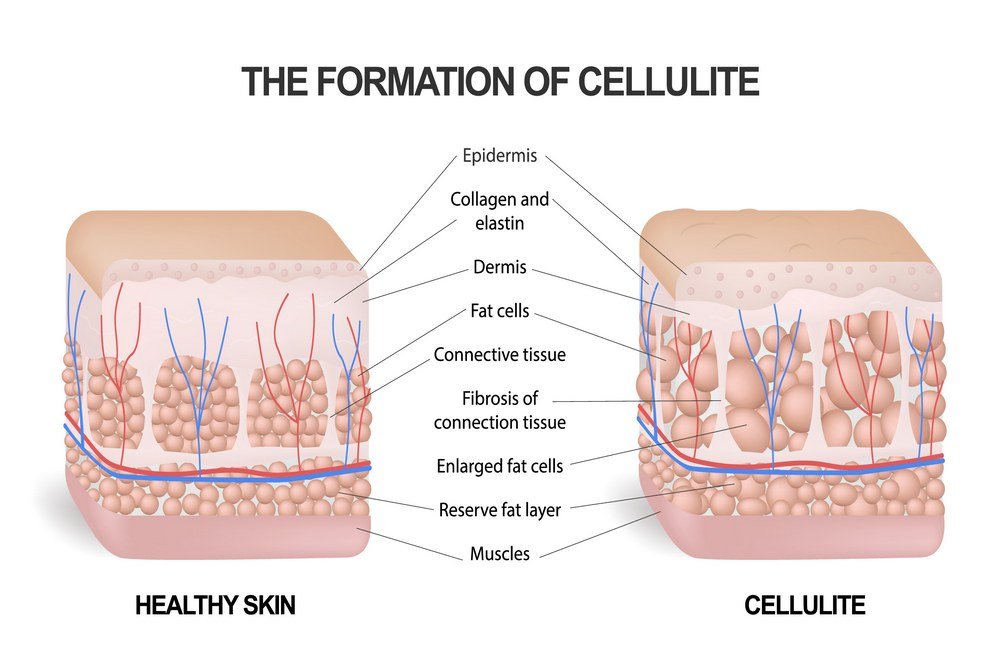
These signs can be investigated in more detail based on histopathology. As evidenced by the ongoing researches on the topic, we find that there is a significant remodeling of fat cells that make up the subcutaneous fat layer and also of the mesh-work of collagen and connective tissue fibers that function as a cage to contain this fat layer. These fibers divide the fat layer into segments comprising globules of fat cells and tug on the skin between these segments. This gives rise to characteristic bumps on the skin. Cellulite differs from simple obesity on similar histopathologic grounds. Obesity is characterized by an increase in size and number of fat accumulating cells called adipocytes. In cellulite, however, a different mechanism is responsible for the characteristic topography of skin. Cellulite involves abundant fat accumulation in lobules which appears as bumps, coupled with thick fibrous septa tethering to the skin and pulling it inwards which appears as depressions.